
Surgical Outcomes
Unless a patient has ongoing spinal cord injury or acute spinal trauma, it is our philosophy that every patient should exhaust non-operative care before considering surgery. Even patients who present with pain and extremity weakness are initially treated with conservative care. In general, we can relieve a person’s pain without surgery more than 90% of the time. Many of the remaining patients cannot be helped with surgery and require ongoing pain management. We often have to tell patients who have extreme spine pain that they are not surgical candidates. It is not uncommon for us to spend a significant amount of time talking a patient out of surgery. As much as we would like to help everyone with surgery, the reality is that there are only a select group of patients who will do well with surgery.
Fortunately, there are specific cases when a person’s pain can be permanently relieved with an operation to treat a structural problem in the spine. Some operations are larger than others. Surgery can range from a 40-minute outpatient decompression procedure to a four- to six-hour multi-level fusion operation. We always seek to leave the smallest surgical footprint possible to fix the problem. However, certain patients do require fusion operations particularly in the setting of instability or scoliosis (curvature of the spine) to give mechanical stability to the spine. We make every effort to be minimally invasive when possible but do have the capability of doing more extensive surgery when necessary.
It is up to the surgeon’s expertise to determine whether a patient is a good candidate for surgery as well as the type of surgery to perform. We believe that the key to getting good surgical outcomes is patient selection and surgical skill. Spine surgeons, like any other skill-based profession, are highly variable. We encourage all patients, regardless of the surgeon they choose to ask surgeons what their surgical outcomes are. We feel that it is unacceptable for a surgeon to subjectively say to a patient, “All of my patients do well and have great outcomes from surgery.” Even in the best of hands with the perfect surgical indications, this is simply false.
One of the biggest components of our practice is the development of a spine surgery outcomes registry. We believe that transparency of surgical outcomes in a field where patient’s perception is often clouded by social influence and aggressive unindicated surgery is critical. The data should speak for itself.
Tracking outcomes following spinal surgery is not subjective and is done with a series of standardized outcome questionnaires. These outcomes are specific to neck or back surgery. Such questionnaires have typically been collected only for clinical research studies or studies for the FDA. However, their use will be increasingly utilized to provide information that can be used to improve surgical results. The outcome surveys are filled out by the patient before getting surgery and at the six-week, three-month, six-month, and one-year time-point following surgery. We utilize a web-based data collection system called www.kareoutcomes.com to manage the data. The current database has grown to include over 700 patients.
Based on this objective data, we can report that:
- 93% of patients who have neck or back surgery for arm or leg pain have some reduction in their pain
- 95% of patients would choose to have surgery again if they had the same problem
This database also allows us to give patients who are considering surgery a “Surgery Specific Report Card” of how other patients who have been operated on by us did after surgery. When our patients ask us what our surgical outcomes are, we show them objective data. An example of specific outcomes for surgery performed by this practice is in the tables below. We are proud of our results and believe that it is a combination of careful patient selection and state-of-the-art surgical technique.
These are the results of a Microdiscectomy procedure, commonly performed for leg pain. This table shows that the average leg pain score was 6.3 before surgery and 1.3 following surgery.
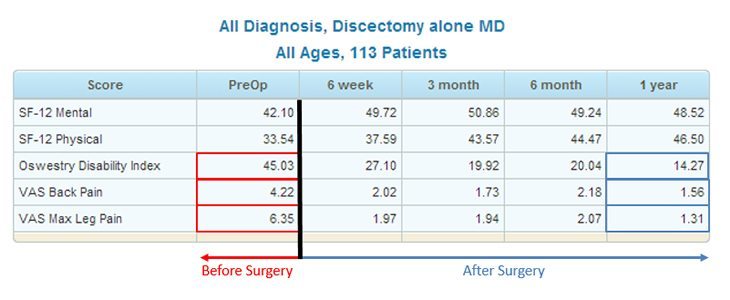
- Oswestry Disability Index (A higher number indicates more disability)
- VAS Back Pain (Ranges from 0–10 with 10 being the worst pain in your life)
- VAS Max Leg Pain (Ranges from 0–10 with 10 being the worst pain in your life)
These are the results of a Lumbar Fusion procedure, commonly performed for leg pain as well as instability or scoliosis of the spine. This table shows that the average leg pain score was 6.5 before surgery and 1.9 following surgery.
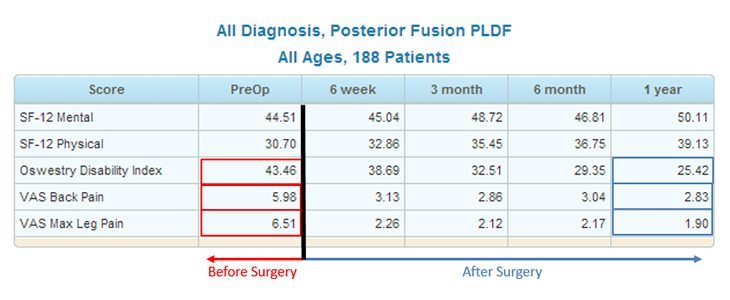
- Oswestry Disability Index (A higher number indicates more disability)
- VAS Back Pain (Ranges from 0–10 with 10 being the worst pain in your life)
- VAS Max Leg Pain (Ranges from 0–10 with 10 being the worst pain in your life)
These are the results of an Anterior Cervical Decompression and Fusion procedure, commonly performed for neck and arm pain. This table shows that the average arm pain score was 6.1 before surgery and 2.3 following surgery.
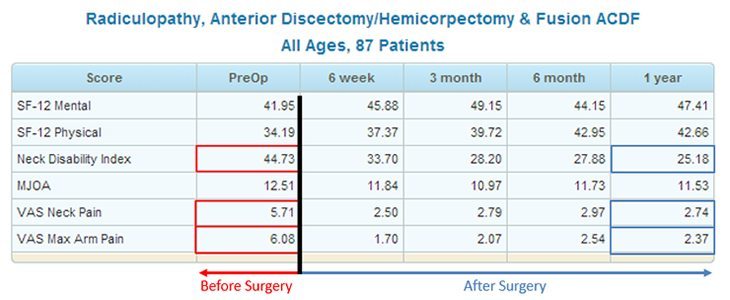
- Neck Disability Index (A higher number indicates more disability)
- VAS Neck Pain (Ranges from 0–10 with 10 being the worst pain in your life)
- VAS Max Arm Pain (Ranges from 0–10 with 10 being the worst pain in your life)
Surgical Patients
If you have surgery scheduled with Dr. Su, there are several forms that need to be completed before surgery that you received during your office visit to schedule surgery. As a convenience, we have included these forms at the bottom of the following page.
Clinical Trials
Please enquire with Dr. Ramana Naidu regarding any current clinical trials he is enrolling.